
| PSMA-directed molecular imaging in prostate cancer PET / CT examination with 68 Ga-PSMA ligands
A new, highly sensitive marker for PET / CT has now been introduced at the Clinic for Nuclear Medicine at Saarland University Hospital in Homburg in order to identify tumor foci in patients with prostate cancer more precisely. The radiopharmaceutical gallium-68-PSMA ligand binds to prostate-specific membrane antigen (PSMA) on the surface of tumor cells and thus enables imaging with very high contrast. In the process, the smallest tumor settlements can be discovered that could escape conventional imaging.
How does the investigation work? A small amount of the gallium-68 labeled PSMA ligand ( 68 Ga-PSMA) is injected into a vein for examination. After the injection, the 68 Ga-PSMA will reach the diseased tissue via the blood vessel system and accumulate significantly more in the diseased cells compared to normal tissue. In order to observe and visualize this distribution in the body, the PSMA was labeled with a short-lived radioactive substance (Gallium-68) before the injection. Its physical half-life is only 68 minutes. The PSMA will increasingly accumulate the diseased tissue. With the help of the PET / CT scanner, the enrichment site can be localized by means of the radiation from the Gallium-68, and the tissue sought can be depicted graphically. In order to enable a reliable assignment to known structures (lymph nodes, soft tissues), a computed tomography is additionally carried out and the 68 Ga-PSMA PET images are superimposed with the CT images and evaluated together (PET / CT). Foci found in PET can thus be precisely assigned to the respective anatomical structures.
documents Please bring all relevant documents with you to the examination (in particular pictures and findings from previous examinations, also in digital form on CD and doctor's letters). For possible intravenous contrast medium administration as part of CT (computer tomography), please have your family doctor determine the creatinine value in the blood as soon as possible - ideally in the week before the examination. The result of the blood test should guide you.
examination procedure
The PET-CT device is open upwards (towards the head) and downwards (towards the legs) and cannot be compared to a tube. If there is pronounced “claustrophobia” (claustrophobia), an anxiety-relieving premedication may be necessary or advisable. Please keep in mind that you are not roadworthy with such an anxiolytic medication on the day of the examination! In the absence of persistent “claustrophobia” (99% of cases), no such medication is required and you can also drive yourself accordingly (before and after the examination).
Side effects: No side effects are expected from the injection of the radioactive tracer itself. Side effects can result from the administration of iodine-containing contrast medium in the context of any accompanying contrast medium-assisted CT (intolerance reaction, hyperthyroidism, aggravation of pre-existing renal insufficiency). If you have had a contrast medium reaction in the past (reddening of the skin, itching, swelling, shortness of breath, etc.), please be sure to point this out to our doctors during the patient's medical consultation.
Radiation exposure: The radiation exposure (radiation exposure) by the gallium PSMA is approximately in the range of twice the natural annual radiation dose (approx. 4-6 mSv). It is below the radiation dose of most conventional CT examinations. Acute and / or chronic radiation damage from gallium PSMA is not expected or has been observed.
Documents to bring Please bring your current documents with you to the examination, eg a CD / DVD with the image data of your current computed tomography or MR examination. Before each PET / CT examination, your family doctor should take a blood sample and determine the values for "creatinine" and "TSH". We kindly ask you to bring them to the examination.
Important: You do not have to be fasting on the day of the examination . You can have a light breakfast. The radiopharmaceutical is made for the patient and cannot be stored. It is imperative to keep your appointment or to inform us in good time if you do not show up .
| DURATION & PRICE |
You can send your findings to Dr Ezziddin via addresses in the link below, asking for comments or a second opinion:
Please enclose the following findings
|
PSMA-directed Radionuclide Therapy (PSMA-PRRT, PRLT) incl Actinium-225 and Lutetium-177Prostate cancer is the most common malignant tumor affecting men in Germany. After local therapy (surgery and/or radiation) with the intention of curing advanced (metastatic) prostate cancer, a supplementary anti-hormone therapy is often initiated. After prolonged anti-hormone therapy (androgen-deprivation therapy, ADT), the tumor cells often become resistant, so that other chemotherapeutic treatment options are used as the tumor disease progresses. The uro-oncologists use the entire range of therapies for advanced prostate carcinoma. PSMA-directed radionuclide therapy, also known as PSMA-directed peptide receptor radionuclide therapy (PSMA-PRRT or PRLT), is a new targeted therapy for patients with advanced prostate carcinoma. PSMA (prostate-specific membrane antigen) is a protein receptor that is richly present on the cell surface of prostate carcinoma cells. This is used for diagnostic and therapeutic procedures in Nuclear Medicine particularily for this tumor entity by means of theranostics, a radioactive nuclide coupled to a substance that binds to PSMA, which emits either detectable radiation for diagnostic purposes or (therapeutically) short-range harmful radiation (e.g. Lu177). During PSMA-directed radionuclide therapy, the radioactive radiation (ß-radiation) exerts its therapeutic effect directly on the tumor cells exposing minimal radiation on the surrounding healthy tissues.
Case Report I PSMA-Therapy 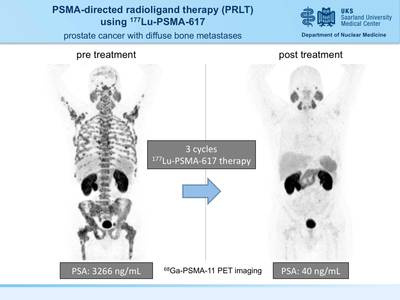 61y old male prostate carcinoma patient with bone metastases. Patient had progressive disease under ADT and abiraterone plus prednisolon. Three treatment cycles of PSMA-directed radioligand therapy (PRLT) using Lutetium-177 PSMA-617 resulted in a dramatic decline of PSA level. Follow-up therapy monitoring by 68Ga-PSMA-11 PET imaging showed only minor residual disease. Indications for PSMA-directed radionuclide therapy (PSMA-PRRT, PRLT) with 177Lu (Lutetium) and/or 225Ac (Actinium) Initially, the prostate carcinoma is usually surgically removed or irradiated with curative intent. Although the therapy is optimal, recurrence often occurs during the further course. If inoperable, this can usually be controlled for an extended period of time with anti-hormonal therapy (ADT, directed against prostate carcinoma-stimulating androgens). The tumor cells finally become insensitive (resistant) to these agents and continue to grow unhindered. Solely bone involvement often offers the possibility of bone-directed radionuclide therapy (Alpharadin, Xofigo). If this therapy is out of question or no longer effective, many patients will have to undergo chemotherapy. Although this can lead to side effects for the patient, it often leads to tumor control for some time. When the tumor cells finally become resistant to this treatment, PSMA-PRRT (PRLT) often still works because it provides targeted intense radiation of the tumor from the inside, sparing the healthy surrounding tissue because of the milimeter or submilimeter range of radiation. This is a new treatment method for patients for whom no satisfactory therapeutic alternatives are left. For an effective treatment, the metastases or tumor lesions should have the ability to accumulate PSMA in sufficient intensity. To determine this, a 68Ga PSMA PET/CT examination is performed as part of the theranostic concept prior to therapy. This PET-CT study is also offered by our department.
Homburg Concept of Tandem 225Ac (Actinium) and 177Lu (Lutetium) PSMA Radioligand Therapy (Alpha/beta Tandem PRLT) We were able to show, that patients developing Lutetium (177Lu) refractory mCRPC desease, i.e. metastatic prostate cancer with insufficient response to 177Lu PRLT, may respond well to 225Ac-augmented 177Lu-PRLT. With our approach we use a low amount of activity of 225Ac together with standard 177Lu activities achieving superior remission rates with less toxicity as the standard 225Ac PRLT (mono Actinium PRLT) approach. Case Report II PSMA-Therapy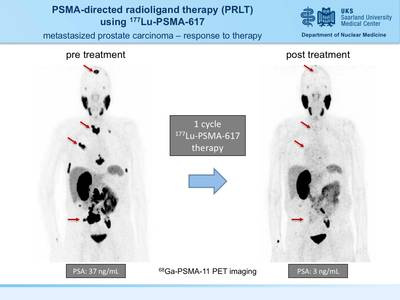 A 77y old male prostate carcinoma patient showed progressive disease after enzalutamide and chemotherapy. Near complete remission after a single treatment of PSMA-directed radioligand therapy using Lutetium-177 PSMA-617. Therapy monitoring was performed by 68Ga-PSMA-11 PET imaging. Therapy procedure Following the preparing examinations (blood tests, quantitative assesment of organ functions, e.g. renal function, salivary gland function), the radionuclide substance is infused through the arm vein at a dose based on the tumor load and the test results. Prophylactic cooling maneuvers of the salivary glands (cooling of the parotid glands from outside) are performed, assuming appropriate for the patient's benefit. Also the infusion of fluids is provided for sufficient hydration (rinsing) . During the inpatient stay, the radiation dose reached in tumor and the sensitive organs (especially kidney) is calculated. This is achieved by serial whole-body and SPECT-CT examinations, which allow quantification of the gamma radiation emitted out from the respective tissue. These measurements also involve blood sampling. The duration of the inpatient stay ranges from 2-4 days.
Side effects In most cases the therapy is very well tolerated. Most patients do not report any noticed side effects. Occasionally there are adverse effects such as minor nausea or reduced appetite for days, taste disturbances or dry mouth (transient or permanent) as well as fatigue. The PSMA-binding radiopharmaceutical is excreted by the kidneys, liver and gallbladder. A normal intestinal activity is therefore required, otherwise stimulation of bowel movements may be considered. A minimum intake of liquids is necessary to ensure this. Liver and kidney values are checked further after therapy. The organs susceptible to radiation-induced injury during this therapy are mainly the salivary and lacrimal glands, which are also rich in PSMA. Cooling of the salivary glands can possibly decrease the severity of radiation damage by means of decreased blood flow in these tissues. Nevertheless, the risk of permanent damage with loss of function (dry mouth) appears to be low with Lu-177 PSMA-PRRT unlike with other radionuclide therapies involving the salivary glands. However, the long-term side effect of dry mouth and/or dry eye cannot be entirely excluded. In addition, this treatment may lead to temporary changes in blood counts.
Case Report III PSMA-Therapy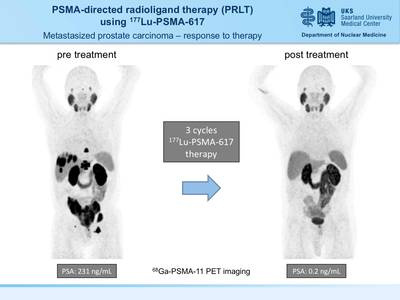 84y old male prostate carcinoma patient with liver and bone metastases (mCRPC). Patient had progressive disease after androgen deprivation therapy (ADT), abiraterone/prednisolon, and radiation therapy. Full biochemical response (complete remission) was achieved by 3 treatment cycles of PSMA-directed radioligand therapy (PRLT) using Lutetium-177 PSMA-617. Therapy monitoring was performed by 68Ga-PSMA-11 PET imaging. Expertise in Homburg; Centre of Molecular Radiotherapy, Dep. of Nuclear Medicine, Saarland University The Department of Nuclear Medicine in Homburg with its Centre of Molecular Radiotherapy focuses on innovative theranostic treatment approaches in oncology. Prof. Ezziddin is a well recognized international expert in targeted radionuclide therapy and has developed various concepts for individualized cancer therapy, which is the main focus of his clinical and scientific efforts. His commitment is to optimize the treatment of advanced metastatic or otherwise difficult-to-treat cancer disease. After the introduction of Lu-177 based therapy in 2004, he pursued and published new concepts for increasing the effect, including intra-arterial and augmentation approaches. In order to optimize PSMA-directed radionuclide therapy, the Homburg group strives to take into account the individual binding properties and receptor capacity, the tumor load, as well as the patient's organ functions and excretion kinetics for therapy planning and decision making.
In Homburg, the Ezziddin working group established a standardized dosing scheme for individualized PSMA-directed (PRLT) and Somatostatin receptor-mediated PRRT. This allows for dose-escalation in difficult or highly advanced metastatic disease. Also, augmentation approaches with different anti-tumor substances and alpha-emitters (Ac225) for tandem PRLT have been succcessfully applied as one of the first centres worldwide.
It is important to emphasize that PSMA-PRRT is still an experimental new therapy for which long-term data are scarce. However, the initial results are so promising that this form of therapy cannot be withheld from patients in need. A temporary tumor mass reduction and tumor control is likely in the setting of good tumoral theranostic uptake and accumulation, however, after repeated treatment courses, this procedure may eventually be no longer able to stop tumor progression, as with all other procedures in the (incurable) metastasized stage of prostate cancer.
Requesting PSMA therapy (PSMA-PRRT, PRLT) The decision on PSMA therapy is made together with the treating urologist, oncologist and, if necessary, the experts of the Homburg University Hospital in an multidisciplinary consensus board after all findings are available. | |